tl;dr: About 1 in 8 deaths in 2022 in Canada were caused by COVID-19. Organ damage caused by COVID seems to be persistent. Each time you get COVID, you and your children roll the dice again as to whether you die or get Long COVID. Get boosted, mask (with an N95 respirator) when you’re indoors with others. Get COVID as few times as you can, and if you get it, rest up longer than you think you need to. Push for better (HEPA) air filtering and ventilation (more air interchanges per hour).
It’s been three and a half years since COVID-19 burst into the world consciousness, and ten months since I last wrote about it.
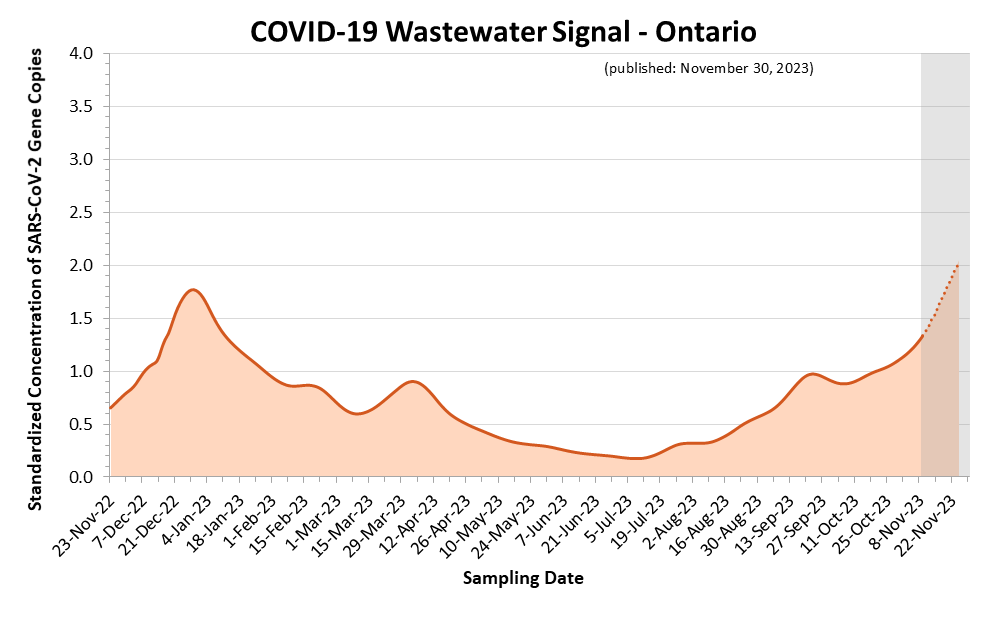
With cases dramatically increasing in North America , and numerous people being ‘surprised that COVID-19 is still a thing‘[1] the time seemed right for an updated review of what we know.
What is COVID-19 and how do you get infected??
COVID-19 is an airborne contagious disease caused by the coronavirus SARS-Cov-2, transmitted from an infected person through inhaled aerosols. These aerosols can linger in indoor air for hours.[2]
How does COVID-19 work?
The SARS-Cov-2 virus affects numerous parts of the body, by attaching its ‘spike protein’ to the ACE2 receptor found in the lungs, heart and cardiovascular system, gastro-intestinal system, and kidneys, causing issues and organ damage in all of those areas.
Longitudinal studies have shown that this organ damage is persistent, with 80-100% of damage present at 6 months still being present at 12 months[2a].
SARS-Cov-2 is also known to have effects on the brain, causing loss of taste/smell and vertigo.[3] Last time, I also reported the UK ‘Brain Bank’ study[3a] which showed ‘detected damage to areas of the brain associated with taste and smell, along with measurable cognitive impact, even when COVID cases which required hospitalization were excluded’, suggesting that even ‘mild’ COVID cases cause brain damage.
In 2022, StatsCan[4] shows that there were about 43 thousand ‘excess deaths’ in Canada (compared to 2019 and earlier), with 18 thousand people specifically confirmed to have died from COVID.
COVID Deaths:
2018 2019 2020 2021 2022 1/x cause Cancer 79,726 80,372 81,242 82,822 82,412 24.67% 4.05 H & Str 67,750 67,081 68,191 68,762 71,272 21.33% 4.69 COVID19 15,890 14,466 19,716 5.90% 16.94 Accid. 15,855 15,527 16,818 19,257 18,365 5.50% 18.19 All: 285,704 285,301 308,412 311,640 334,081 100.00% Excess: 0 0 16,334 21,718 43,378 12.98% 7.70
Given the inaccuracies and delays in reporting deaths[5], and the steadiness of the death rate before 2020 (compare the ‘All:’ line in the table above for 2018/2019 with the much greater variability in 2020/2021/2022), it is generally accepted that ‘Excess Deaths’ is the correct way to measure deaths caused by COVID-19.
With that being said, the numbers paint a sobering picture. While 43,378/38 million (0.11%) may not seem like a large number, 43,378/334,081 is 12.98%. That means that for each person that died in Canada in 2022, there was about a 1 in 8 chance that their death was caused by COVID-19.
Also note that there is a substantial uptick in cardiac (Heart & Stroke) related deaths, especially in 2022. COVID is known to increase the risk of heart attack and stroke, and the ~3,000 excess Heart & Stroke-related deaths in 2022 in Canada help us understand the magnitude of the issue.
COVID-caused chronic diseases ‘Long COVID’:
The prevalence of ‘Long COVID’ is generally accepted to be ‘at least 10%’ , with an estimated 65 million people affected worldwide, with that number increasing daily.[2a1]
Last time, I shared a study[2b] done with data from Veteran’s Administration patients from the U.S., showing that COVID reinfection is just as dangerous (equal chance of death) or more dangerous (increased chance of hospitalization).
While this clearly showed additive effects from second COVID infections, this was a very specific (and not very healthy) cohort.
Since then, there was a study in the UK which looked specifically at the incidence of Long COVID after first and second infections. Among those >=16yo, ‘Activity-limiting’ Long COVID was reported by 2.8% after first infection, with an additional 1.6% after second infection, showing that the effects are either additive, or somewhat random with each infection. Those <16yo had an incidence of 0.6% after first infection, with an additional 0.4% after second infection. The above show that second (and subsequent) infections are still dangerous, still causing life-changing illness, including in children. Even if children may not show the effects as often, they are still affected, and subsequent infections can and do still cause Long COVID in children. So, given the current high COVID rates (see the Ontario graph above), what actions should you take to protect yourself? Wear a good mask: The chart below is from a study performed pre-Omicron, but the general message holds. A cloth or surgical or KN95 (earloop) mask is better than nothing, but not really very helpful unless everyone is wearing one. Specifically, the times below should be revised downward, probably significantly, but even the author has not done so because they don’t know how far to revise them.
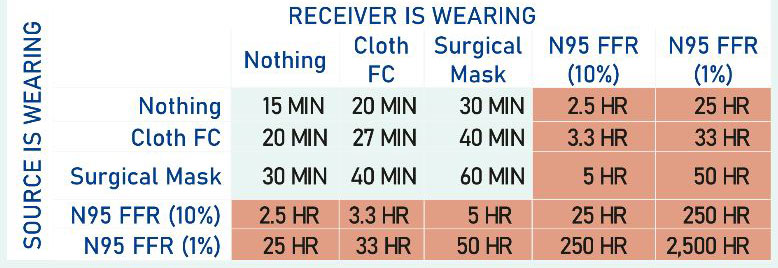
If you want to actually protect yourself, you need an N-95 or better (ideally fit tested). My favourite is this one from 3M, as the headloop bands are a mixture of cloth and elastic, and are thus less likely to break.
Check (and improve) the ventilation:
A CO2 monitor such as the Aranet can very quickly tell you how well-ventilated your area is. Anything around 500ppm means that the air in your space is ‘like outside’.
The CDC recommends at least 5 air changes per hour. You can ask your local HVAC expert for the stats on the system where you live or work.
Continue to get vaccinated/boosted:
Vaccinations have been shown to reduce the likelihood of death and long covid[6]
Should you get the next COVID booster?
Health Canada & Toronto Public Health recommend staying up to date with your vaccines (Health Canada says every 6 months, others may recommend more frequently).
If so, which one?
The updated XBB-specific vaccine is known to give a stronger immune response to the more recent variants. Toronto Public Health also has more detailed guidance based on the age of the individual and which vaccines/boosters they have already received.
Should you get the flu shot? If so, how do you time it vs. the COVID booster?
Thanks for reading this far. Working together, we can get through this, but it might get worse before it gets better, until we as a society decide that we actually want to solve this. Stay safe out there.
[1] Twitter announcement that Colbert will be isolating for a few more days.
[2] “Small saliva aerosols (<50 μm) may remain suspended in the air for hours, during which any viable virus is estimated to gradually decrease. Insights into the evaporation characteristics of saliva droplets and aerosols: Levitation experiments and numerical modeling, Christian Lieber, Stefanos Melekidis, Rainer Koch, Hans-Jörg Bauer”
[2a] Multi-organ impairment and long COVID: a 1-year prospective, longitudinal cohort study
Andrea Dennis, Daniel J Cuthbertson, Dan Wootton, Michael Crooks, Mark Gabbay, Nicole Eichert, Sofia Mouchti, Michele Pansini, Adriana Roca-Fernandez, Helena Thomaides-Brears, Matt Kelly, Matthew Robson, Lyth Hishmeh, Emily Attree, Melissa Heightman, Rajarshi Banerjee, and Amitava Banerjee
Journal of the Royal Society of Medicine, Volume 116, Issue 3
https://doi.org/10.1177/01410768231154703
[2a1] Long COVID: major findings, mechanisms and recommendations, Hannah E. Davis, Lisa McCorkell, Julia Moore Vogel & Eric J. Topol, Nature Reviews Microbiology volume 21, pages 133–146 (13 January 2023)
[2b] Acute and postacute sequelae associated with SARS-CoV-2 reinfection, Benjamin Bowe, Yan Xie & Ziyad Al-Aly, Nature Medicine volume 28, pages 2398–2405 (Published online 2022 Nov 10)
[3] “The Prevalence of Dizziness and Vertigo in COVID-19 Patients: A Systematic Review“, George Korres,1,* Dimitrios K. Kitsos,2 Diego Kaski,3 Anthi Tsogka,2 Sotirios Giannopoulos,2 Vasileios Giannopapas,4 Giorgos Sideris,1 Giorgos Tyrellis,1 and Konstantine Voumvourakis2
[3a] SARS-CoV-2 is associated with changes in brain structure in UK Biobank, Gwenaëlle Douaud, Soojin Lee, Fidel Alfaro-Almagro, Christoph Arthofer, Chaoyue Wang, Paul McCarthy, Frederik Lange, Jesper L. R. Andersson, Ludovica Griffanti, Eugene Duff, Saad Jbabdi, Bernd Taschler, Peter Keating, Anderson M. Winkler, Rory Collins, Paul M. Matthews, Naomi Allen, Karla L. Miller, Thomas E. Nichols & Stephen M. Smith, Nature volume 604, pages 697–707 (07 March 2022)
[4] Most recent full-year data, sources: Excess Deaths, Excess Deaths detailed data, Confirmed Deaths by Cause of Death (including Confirmed COVID Deaths).
[5] Many sources, but the most official one: https://www.statcan.gc.ca/en/subjects-start/health/life_expectancy_and_deaths/faq
[6] Effect of covid-19 vaccination on long covid: systematic review
Oyungerel Byambasuren,corresponding author1 Paulina Stehlik,1 Justin Clark,1 Kylie Alcorn,2 and Paul Glasziou1
BMJ Med. 2023; 2(1): e000385.
Published online 2023 Feb 1. doi: 10.1136/bmjmed-2022-000385
PMCID: PMC9978692
PMID: 36936268
Tab count: 98
Papers which didn’t make the cut:
“Transcriptional reprogramming from innate immune functions to a pro-thrombotic signature by monocytes in COVID-19”
https://www.nature.com/articles/s41467-022-35638-y
(linked by WesElyMD https://twitter.com/weselymd/status/1610257204090896385? )
“The prevalence and long-term health effects of Long Covid among hospitalised and non-hospitalised populations: a systematic review and meta-analysis”
https://www.thelancet.com/journals/eclinm/article/PIIS2589-5370(22)00491-6/fulltext
“Long COVID after breakthrough SARS-CoV-2 infection”
https://www.nature.com/articles/s41591-022-01840-0
“Development of a Definition of Postacute Sequelae of SARS-CoV-2 Infection”
https://jamanetwork.com/journals/jama/fullarticle/2805540
“Long COVID: major findings, mechanisms and recommendations”
https://www.nature.com/articles/s41579-022-00846-2
” Three in five long COVID patients have organ damage a year after infection”
https://www.downtoearth.org.in/blog/health/three-in-five-long-covid-patients-have-organ-damage-a-year-after-infection-87848
“COVID-19 and multiorgan failure: A narrative review on potential mechanisms”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC7533045/
“Long covid outcomes at one year after mild SARS-CoV-2 infection: nationwide cohort study”
https://www.bmj.com/content/380/bmj-2022-072529
“Does the risk of getting long Covid increase each time you get reinfected?”
https://www.statnews.com/2023/09/20/do-long-covid-odds-increase-with-second-infection/
(Interview with one of the authors of the VA study linked above)
“SARS-CoV-2 Reinfections and Long COVID in the Post-Omicron Phase of the Pandemic”
https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10454552/
“Long COVID and Significant Activity Limitation Among Adults, by Age — United States, June 1–13, 2022, to June 7–19, 2023”
https://www.cdc.gov/mmwr/volumes/72/wr/mm7232a3.htm