So, we just watched Oppenheimer today. I’d been resisting it, because despite[1] all the hype, I didn’t really see the point; I didn’t really see why I specifically needed to watch it[2]. However, S really wanted to watch it together, and it was now out on home video[3] so we sat down for a nice holiday Tuesday matinee[4].
First off, it was fantastic, really well done. If you haven’t seen it yet, please pause this read, do so, and then come back here.
[Spoilers beyond this point]
It’s interesting that I feel I have to talk about spoilers here, for a historical/biographical movie. But I do need to. Anytime there’s a biopic, there are choices about what is shown on-screen, and how each of those things are sequenced and portrayed. The flashback structure and eventual reveal at the end was really good for building and releasing the dramatic tension (the music was fantastic for this…especially the completely silent atomic bomb explosion, which was fantastically effective, along with dramatically representing some of the delay between seeing and hearing such an event caused by the difference between the speed of sound and light).
I’d always conceptualized the Manhattan Project through the eyes of Feynman, from his essay ‘Los Alamos from Below'[5]. I think it wasn’t until today that I really understood that he really meant it that way. I had always seen Oppenheimer as the leader/front man who had to exist so that the project could happen, but also as a quasi-mythical distant figure. I’d also conceptualized the ethical dilemmas about actually building a nuclear device as being shared and agonized over by each and every one of the scientists and engineers (and everyone) at Los Alamos.
The Oppenheimer story, being a biopic largely of one person, centralized a lot of that in one person (Oppenheimer). Interestingly, the movie tried really really hard (and I think succeeded) at leaving Oppenheimer a complex character, with multiple possible interpretations of many of the very real decisions he made along the way.
Cillian Murphy was fantastic, it seemed to me having some of the ‘dazed at the enormity of what we’re doing’ present at all points of the movie, which is appropriate for flashbacks, or perhaps for someone who had his head in the clouds of physics his entire life[6].
Having not seen much about the movie (aside from a clip or two, and hearing about how Cillian Murphy prepared for the role[7]), I wasn’t expecting what type of movie it was, or how pivotal a role Robert Downey Jr.’s character was to play (or that he was to be the villain). He had mentioned in an interview that Nolan had asked him to play against type[8] compared to many of his recent characters.
Florence Pugh was fantastic, although it’s hard to top her iconic performance as Yelena Belova. Matt Damon was an excellent potty-mouthed general, and Emily Blunt and the rest of the supporting cast were great.
I thought it was a really nice touch having Einstein and Bohr both mention that they were from the previous generation, and that this problem was not theirs, but fully belonged to Oppenheimer. S mentioned in particular that it was interesting to see a different, older/more bitter side of Einstein, rather than the ‘genius’.
I also appreciated for the nods to Copenhagen (the play), where Bohr mentions that he got significant information from Heisenberg, and a disturbing scene where Oppenheimer meets Heisenberg, and then immediately turns away and leaves, presumably because he (a Jewish boy from New York) senses that Heisenberg would be willing to work on a Bomb for Hitler[9].
There was also just enough of a Feynman cameo, with two shots of him playing the bongos. With his charisma and fame, anything more might have upstaged the rest of the movie.
Great movie. See it if you haven’t. Let me know what you think!
[1] Or perhaps because of it. I’m often somewhat contrarian about things like that.
[2] Interestingly, I perceived that I needed to see Barbie more than Oppenheimer, but that’s a story for another time.
[3] How anachronistic is the phrase ‘home video’ now?
[4] I find many/most movies emotionally draining/exhausting, and they often require significant processing time afterwards (and this was no exception), and it’s really nice to still have some sun out after the movie is over, which somehow helps with this.
A few days ago, I posted about some chilling COVID statistics[1], and said that each time you get COVID, you and your children ‘roll the dice’ (referring to the relatively high probability of death and/or organ damage/disability).
A friend of mine commented that this was ‘loaded language and emotional rhetoric’, and it came ‘across as an attempt at manipulation or a genuine reflection of fear felt by the author’.
Setting aside the obvious ‘loaded dice’ pun[2], I’d like to interrogate the meaning of ‘rolling the dice’ (and also the use of such rhetorical flourishes in a Health and Safety context).
Colloquially, I’ve always thought of it in the second sense given by Miriam-Webster: “It’s a roll of the dice whether we succeed or fail.”, meaning that we are not in control of the outcome, and you should be prepared for the high chance of negative outcome.
Of course, ‘high chance’ is defined differently by different people, and in different situations, people having different risk thresholds than each other, and at different times. For example, a 1 in 10 chance of the bottom of your sock becoming wet[4] is very different than a 1 in 10 chance of being hit by a car.
For the sake of argument, let’s compare the above usage of ‘rolling the dice’ with the most popular[5] dice betting[5a] game ‘Craps‘. In Craps, the two most well known[6] sets of odds are ‘Pass’, or ‘will you win this set of rolls’, and winning on the first roll.
Winning on the first roll in Craps requires rolling either a ‘7’ or an ’11′[8], for a total probability of 8/36, or about 22%. Many might think that rolling a 7 is the way to win in Craps (it’s also one way to lose, if your first roll was 4,5,6,8,9,10). Rolling a 7 has a probability of 6/36, or about 17%.
One could also argue that ‘a roll of the dice’ is rolling one six-sided die[9], but that just gives us the 1 in 6 or ~17% chance above again. Higher (or lower) order polyhedral dice[10] (or larger numbers of dice) can give us arbitrarily different odds, but let’s stop here.
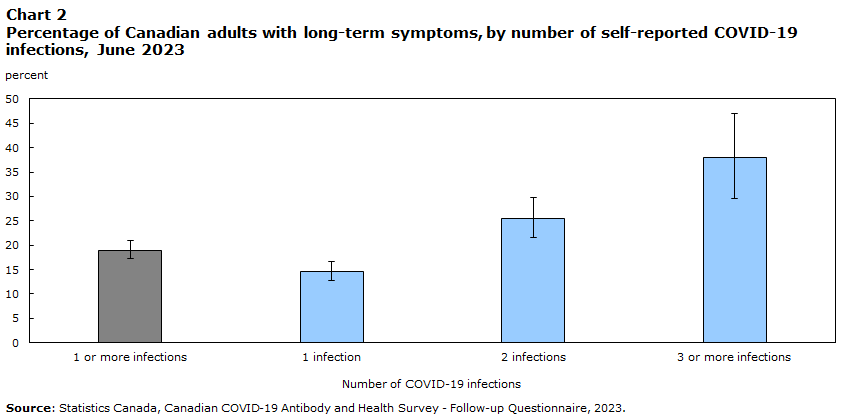
Today, Statscan reported on the prevalence and ‘Experiences of Canadians with long-term symptoms following COVID-19’.
“As seen in Chart 2, Canadians reporting two known or suspected COVID-19 infections (25.4%) were 1.7 times more likely to report prolonged symptoms than those reporting only one known or suspected infection (14.6%), and those with 3 or more infections (37.9%) 2.6 times more likely. ” https://www150.statcan.gc.ca/n1/pub/75-006-x/2023001/article/00015-eng.htm
This shows that about 14.6% reported long-term symptoms after one infection (about 1 in 7), then of the remaining 85.4%, about one in 8 developed long-term symptoms after a second infection, then of the remaining 74.6%, about one in 6 developed long-term symptoms.[11]
Each of these is pretty close to ‘a roll of the dice’, as we defined above.
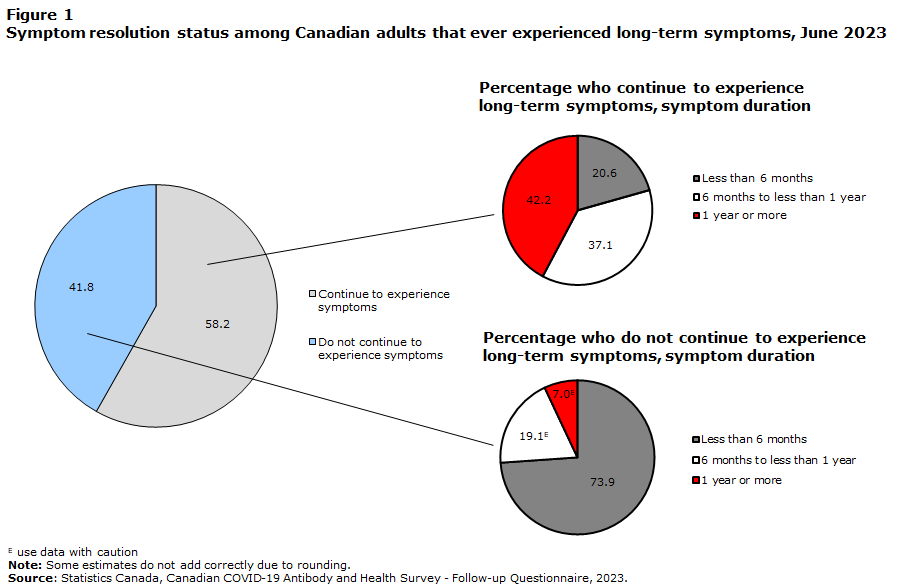
Perhaps more disturbing is that more than half of those who reported long-term symptoms reported no improvement in those symptoms over time:
“Almost half of Canadians who reported that they continue to experience long-term symptoms also reported no improvement over time” “Many Canadians with long-term symptoms experience a protracted symptom duration. As of June 2023, 58.2% of infected Canadians who ever reported long-term symptoms continue to experience them. Among Canadian adults who continued to experience long-term symptoms, 79.3% had been experiencing symptoms for 6 months or more, including 42.2% with symptoms for one year or more (Figure 1).” https://www150.statcan.gc.ca/n1/pub/75-006-x/2023001/article/00015-eng.htm
Also, more than 1 in 5 of those with persistent symptoms (600,000 Canadians) missed days of work or school, missing an average of 24 days each.
Having shown that this is a reasonable use of the phrase ‘roll of the dice’, I also wanted to address the idea of using emotional appeals in public education about health and safety.
A number of years I had the privilege of attending safety training run by Minerva Canada, where a talk was being given by a representative from a car manufacturing company that you’ve heard of. He was talking about their ‘getting to zero’ workplace accidents project, and he mentioned that at some point, after you’ve tried asking people nicely enough times, you have to get the ‘300 lb gorilla to go tell the guy to wear his @#$%ing safety harness’.
That was my sixth and this will be my seventh post talking about the dangers of COVID. At some point, using stronger (but still accurate) language to educate people about the dangers they and their children face due to action or inaction becomes necessary if we actually want to solve the problem.
[1] “tl;dr: About 1 in 8 deaths in 2022 in Canada were caused by COVID-19. Organ damage caused by COVID seems to be persistent. Each time you get COVID, you and your children roll the dice again as to whether you die or get Long COVID. Get boosted, mask (with an N95 respirator) when you’re indoors with others. Get COVID as few times as you can, and if you get it, rest up longer than you think you need to. Push for better (HEPA) air filtering and ventilation (more air interchanges per hour).” link to post
[5a] I mention the ‘most popular dice betting game’ partially because most people will have a passing familiarity, I know some of the odds, and those odds are easy to explain. Compare with the games on the ‘top 10 all-time best-seller list‘: Monopoly (3), Clue (5) (uses one six-sided die for movement, but the deduction and knowing your opponents is far more important for gameplay), and Backgammon (8)
[6] I admit, most well known to me, based on learning about Craps during a probability module in high school. There are a large number of ‘standard’ betting options in Craps, but I suspect most people will not have heard of most of them.
[11] Here, I’m assuming that each time a person catches COVID, they either progress into Long COVID, or stay ‘long-term unaffected’. This allows modeling of each subsequent infection independently. With the numbers above, 1st infection has a ~14.6% chance of leading to Long Covid (1 in 6.85), of the remaining 85.4 people, 25.4-14.6=10.8 of them or 10.8/85.4 = 12.6% or 1 in 7.9, then of the remaining 74.6 people, 37.9-25.4=12.5 of them or 12.5/74.6 = 16.8% or one in 5.97. Note that the last number includes those with more than three infections, so one would expect the number for 3 infections to be less than that. Also note that biology is often not linear, and a linear model such as this one may be simplistic, and should only be used for illustrative purposes, no matter how well it fits the curve.
tl;dr: About 1 in 8 deaths in 2022 in Canada were caused by COVID-19. Organ damage caused by COVID seems to be persistent. Each time you get COVID, you and your children roll the dice again as to whether you die or get Long COVID. Get boosted, mask (with an N95 respirator) when you’re indoors with others. Get COVID as few times as you can, and if you get it, rest up longer than you think you need to. Push for better (HEPA) air filtering and ventilation (more air interchanges per hour).
It’s been three and a half years since COVID-19 burst into the world consciousness, and ten months since I last wrote about it.
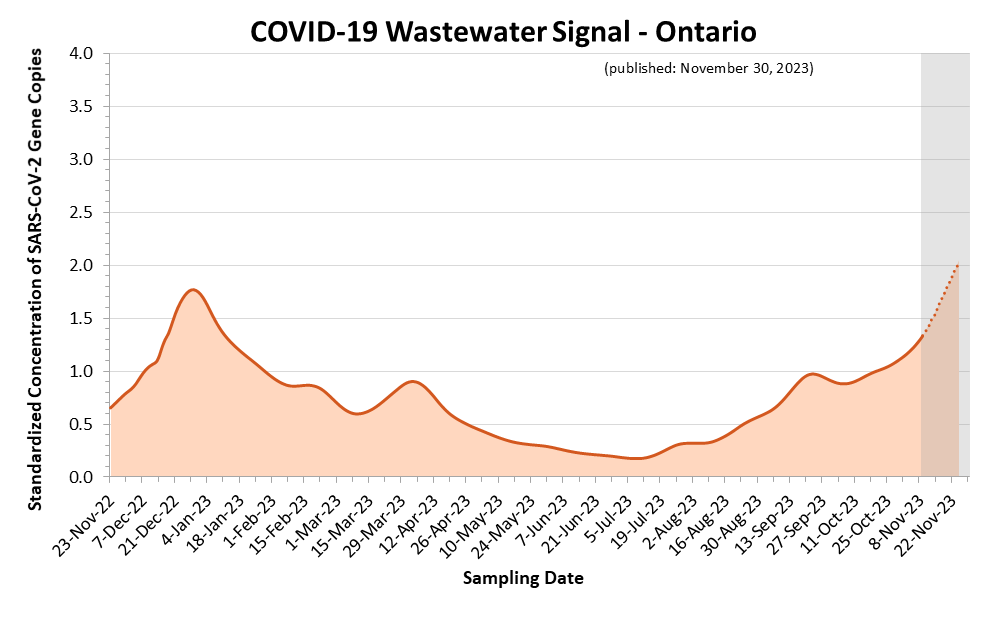
With cases dramatically increasing in North America , and numerous people being ‘surprised that COVID-19 is still a thing‘[1] the time seemed right for an updated review of what we know.
Ontario COVID-19 Wastewater Signal, showing the current (November 2023) peak as the highest in the past 13 months.
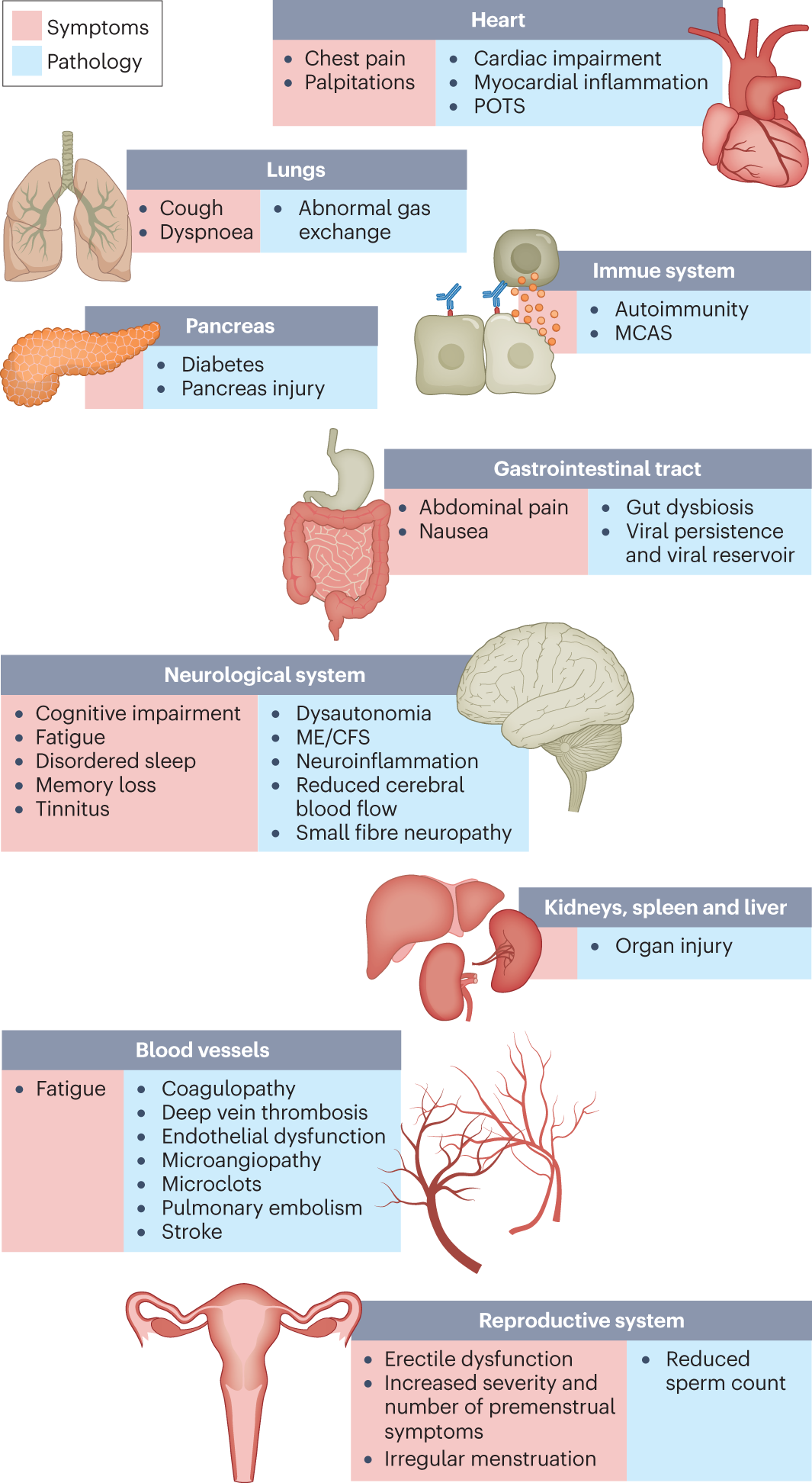
The SARS-Cov-2 virus affects numerous parts of the body, by attaching its ‘spike protein’ to the ACE2 receptor found in the lungs, heart and cardiovascular system, gastro-intestinal system, and kidneys, causing issues and organ damage in all of those areas.
Longitudinal studies have shown that this organ damage is persistent, with 80-100% of damage present at 6 months still being present at 12 months[2a].
SARS-Cov-2 is also known to have effects on the brain, causing loss of taste/smell and vertigo.[3] Last time, I also reported the UK ‘Brain Bank’ study[3a] which showed ‘detected damage to areas of the brain associated with taste and smell, along with measurable cognitive impact, even when COVID cases which required hospitalization were excluded’, suggesting that even ‘mild’ COVID cases cause brain damage.
In 2022, StatsCan[4] shows that there were about 43 thousand ‘excess deaths’ in Canada (compared to 2019 and earlier), with 18 thousand people specifically confirmed to have died from COVID.
Given the inaccuracies and delays in reporting deaths[5], and the steadiness of the death rate before 2020 (compare the ‘All:’ line in the table above for 2018/2019 with the much greater variability in 2020/2021/2022), it is generally accepted that ‘Excess Deaths’ is the correct way to measure deaths caused by COVID-19.
With that being said, the numbers paint a sobering picture. While 43,378/38 million (0.11%) may not seem like a large number, 43,378/334,081 is 12.98%. That means that for each person that died in Canada in 2022, there was about a 1 in 8 chance that their death was caused by COVID-19.
Also note that there is a substantial uptick in cardiac (Heart & Stroke) related deaths, especially in 2022. COVID is known to increase the risk of heart attack and stroke, and the ~3,000 excess Heart & Stroke-related deaths in 2022 in Canada help us understand the magnitude of the issue.
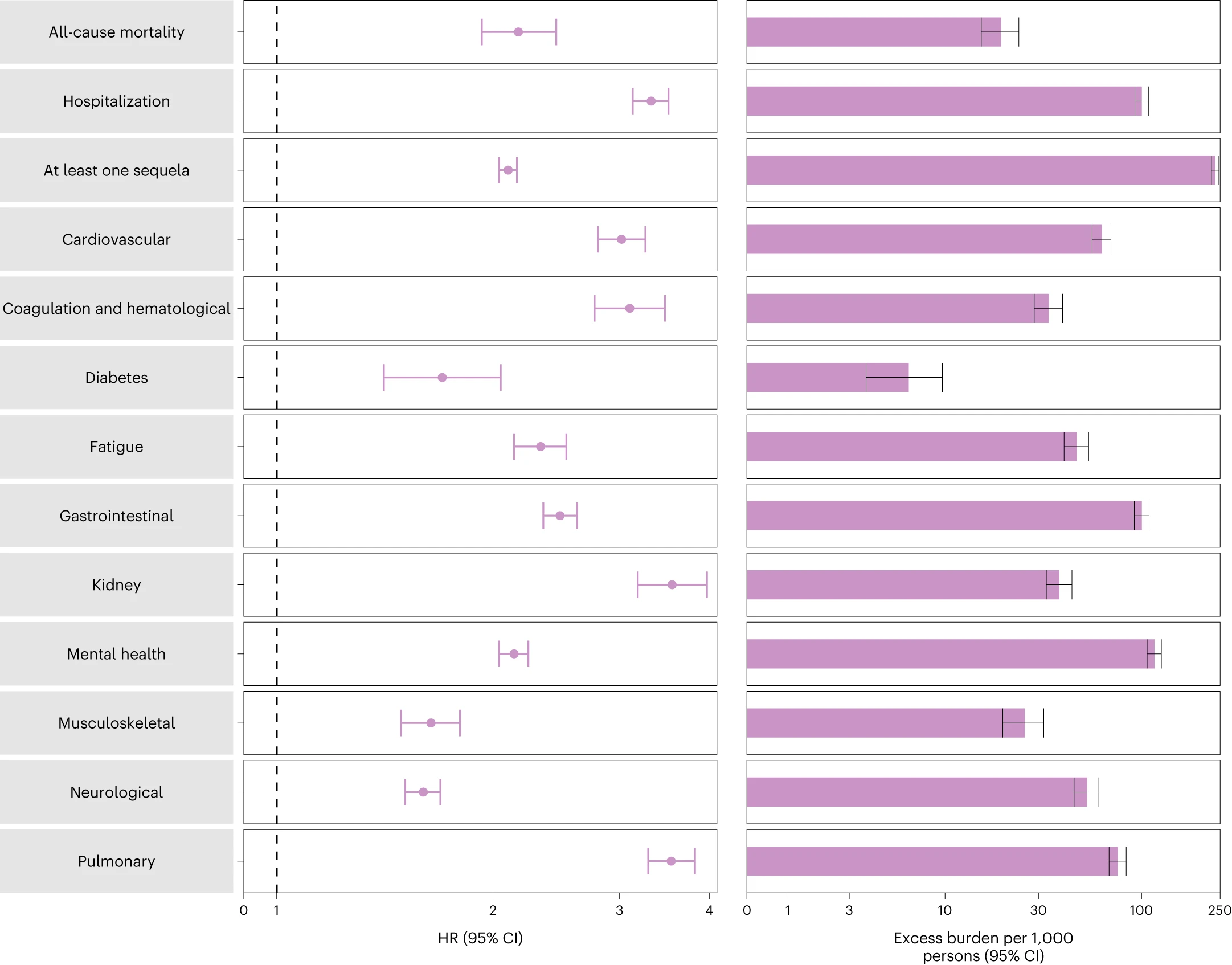
Last time, I shared a study[2b] done with data from Veteran’s Administration patients from the U.S., showing that COVID reinfection is just as dangerous (equal chance of death) or more dangerous (increased chance of hospitalization).
While this clearly showed additive effects from second COVID infections, this was a very specific (and not very healthy) cohort.
Since then, there was a study in the UK which looked specifically at the incidence of Long COVID after first and second infections. Among those >=16yo, ‘Activity-limiting’ Long COVID was reported by 2.8% after first infection, with an additional 1.6% after second infection, showing that the effects are either additive, or somewhat random with each infection. Those <16yo had an incidence of 0.6% after first infection, with an additional 0.4% after second infection.
The above show that second (and subsequent) infections are still dangerous, still causing life-changing illness, including in children.
Even if children may not show the effects as often, they are still affected, and subsequent infections can and do still cause Long COVID in children.
So, given the current high COVID rates (see the Ontario graph above), what actions should you take to protect yourself?
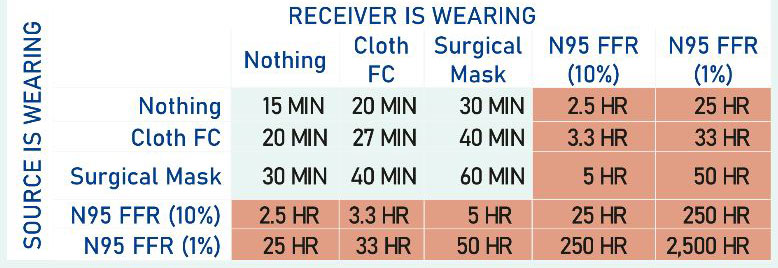
Wear a good mask:
The chart below is from a study performed pre-Omicron, but the general message holds. A cloth or surgical or KN95 (earloop) mask is better than nothing, but not really very helpful unless everyone is wearing one. Specifically, the times below should be revised downward, probably significantly, but even the author has not done so because they don’t know how far to revise them.
COVID Masking Quality Table
If you want to actually protect yourself, you need an N-95 or better (ideally fit tested). My favourite is this one from 3M, as the headloop bands are a mixture of cloth and elastic, and are thus less likely to break.
Check (and improve) the ventilation:
A CO2 monitor such as the Aranet can very quickly tell you how well-ventilated your area is. Anything around 500ppm means that the air in your space is ‘like outside’.
Thanks for reading this far. Working together, we can get through this, but it might get worse before it gets better, until we as a society decide that we actually want to solve this. Stay safe out there.
[2a] Multi-organ impairment and long COVID: a 1-year prospective, longitudinal cohort study
Andrea Dennis, Daniel J Cuthbertson, Dan Wootton, Michael Crooks, Mark Gabbay, Nicole Eichert, Sofia Mouchti, Michele Pansini, Adriana Roca-Fernandez, Helena Thomaides-Brears, Matt Kelly, Matthew Robson, Lyth Hishmeh, Emily Attree, Melissa Heightman, Rajarshi Banerjee, and Amitava Banerjee
Journal of the Royal Society of Medicine, Volume 116, Issue 3
https://doi.org/10.1177/01410768231154703
[3a] SARS-CoV-2 is associated with changes in brain structure in UK Biobank, Gwenaëlle Douaud, Soojin Lee, Fidel Alfaro-Almagro, Christoph Arthofer, Chaoyue Wang, Paul McCarthy, Frederik Lange, Jesper L. R. Andersson, Ludovica Griffanti, Eugene Duff, Saad Jbabdi, Bernd Taschler, Peter Keating, Anderson M. Winkler, Rory Collins, Paul M. Matthews, Naomi Allen, Karla L. Miller, Thomas E. Nichols & Stephen M. Smith, Nature volume 604, pages 697–707 (07 March 2022)
So, I was out for my morning walk today, and it started to rain. Luckily, I had planned ahead and brought my umbrella. I opened it up, and was standing there, enjoying the rain…and then I started to walk, and my legs started to get wet. I stopped, my legs stopped getting wet, I started walking, my legs got wet again.
The question is why?
I narrowed the problem down to the following variables:
– Height of the person (technically, the height of the edge of the umbrella)
– Walking speed and wind speed (I’m putting these together for reasons you’ll see later)
– Size and shape of rain droplets (this is to measure terminal velocity)
– S also added ‘size of umbrella’, but I’ll address that in the assumptions section
This is a lot of variables, so let’s make some assumptions:
– The human in question is about 2m tall (accurate within 5%)
– The edge of the umbrella is about 2m from the ground (accurate within 10-15%)
– The edge of the umbrella is about 25-50cm from the front of the leg horizontally
– We count the leg as getting wet as when the rain hits the front of the leg just above the ground
– Length of a step is about 80cm (as per this page)
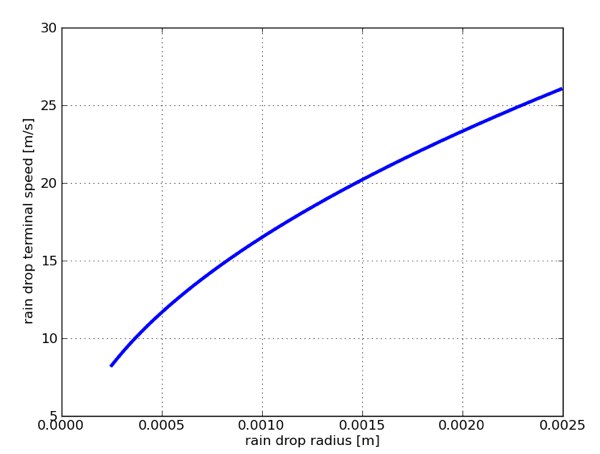
– Raindrop terminal velocity is about 20m/s, as per this graph:
Graph of ‘rain drop terminal speed’ vs. ‘rain drop radius’, from Wired “How Fast Is Falling Rain?”, August 29/2011
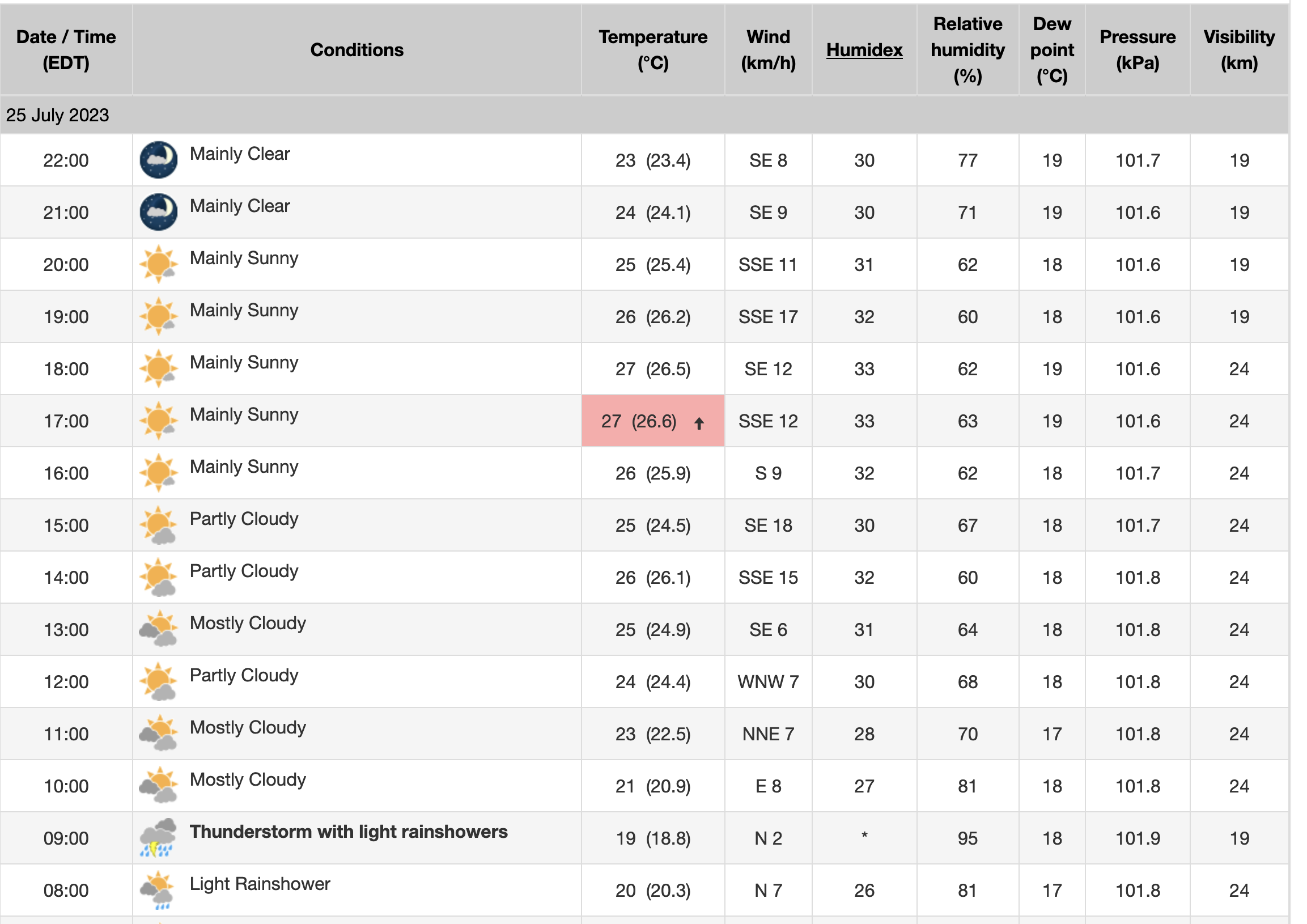
– Wind-speed is negligible, as per this chart from Environment Canada, showing that wind at the time in question (9am) was about 2km/h, from the North:
Table showing weather data for Toronto for 2023-07-25. Relevant part is showing ‘Thunderstorm with light rainshowers’ and ‘Wind 2km/h, N’ at 9am.
Now on to the math!
We can easily show that with negligible wind, rain falling straight down will not hit the legs.
But assuming 90-degrees from ground vertical legs, what wind-speed would be necessary to rain on them?
At 20m/s, the rain would need to travel 0.25m or 0.5m horizontally as it traveled 2m vertically, or a horizontal wind of about 20m/s * 0.25m/2m = 2.5m/s or 9km/h for 25cm of umbrella overhang to 18km/h for 50cm of umbrella overhang.
So it turns out that the wind-speed was actually really important, as you can see that at other points today, it alone would have made the difference.
Now, what happens when we start walking? There are two factors at play here:
– Walking speed
– Extension of the leg forward out of the protection of the umbrella as you take a step
So we have to add some more assumptions:
– Assuming an average walking speed of about 5.4km/h or 1.5m/s
– Assuming that the toe to toe per step distance is 0.8m (from above), assume that at maximum extension, the tip of the leg is 40cm ahead of the body
Using the wind-speed calculation above, we can see that 1.5m/s of forward motion would only counteract about 1.5m/s / 20m/s * 2m = 15cm of umbrella cover, not enough to make your legs wet.
However, if your leg is 40cm ahead of your body, that would be enough if your umbrella was any reasonable amount off ‘exactly centered’ over the front of your body, and if your leg is 40cm ahead, and your walking speed adds another 15cm, that is enough to counteract even perfect vertical umbrella placement (40cm + 15cm > 50cm).
My experience this morning suggests that either the rain was falling more slowly than 20m/s, I was walking slightly faster than 1.5m/s, or I was resting the umbrella diagonally over my shoulder (most likely). This would have given me the approx. 25cm protection above, and caused my legs to be wet only while I was walking.
How would you calculate this? What would your assumptions be? Have you experienced this? Are you going to test this the next time it rains? Are you as surprised as I am that leg placement and step length are much more important than walking speed (as long as you’re only walking)?
tl;dr: Get COVID as few times as you can. Getting COVID the second time is just as likely to kill or disable you as the first time. COVID killed more people in Canada in 2022 than 2020 or 2021, and is disabling many more in an ongoing way. Use masks and better-filtered air to get COVID as few times as you can, and if you do get it, rest up for as long as you can while recovering.
It’s now been more than three years[1] years since COVID-19 entered the world stage, and it’s worth a few minutes to take stock of what we know, where we are, and what we should be doing next.
Acute symptoms vary widely, from respiratory such as cough, fever, shortness of breath, and congestion/sputum, to musculo-skeletal with muscle & joint pain, headache and fatigue, to gastro-intestinal with abdominal pain, vomiting and/or diarrhea. Neurological (separate from nasal congestion) loss of taste and smell is perhaps the most well-known distinctive COVID symptom, made famous by online reviews of scented candles.
These acute symptoms also include death, although the exact number is difficult to measure for a number of reasons[2]. The official ‘Case Fatality Rate‘[3] is generally measured to be around 1%, for example by the John Hopkins dashboard. Taking estimated numbers of non-tested and asymptomatic individuals into account, the actual overall ‘Infection Fatality Rate’ is generally calculated to be between 0.5-1% for ‘wild type’ virus. This rate is modified by age, risk factors, variant of interest (Alpha/Delta/Omicron/XBB1.5/etc), and vaccination status.
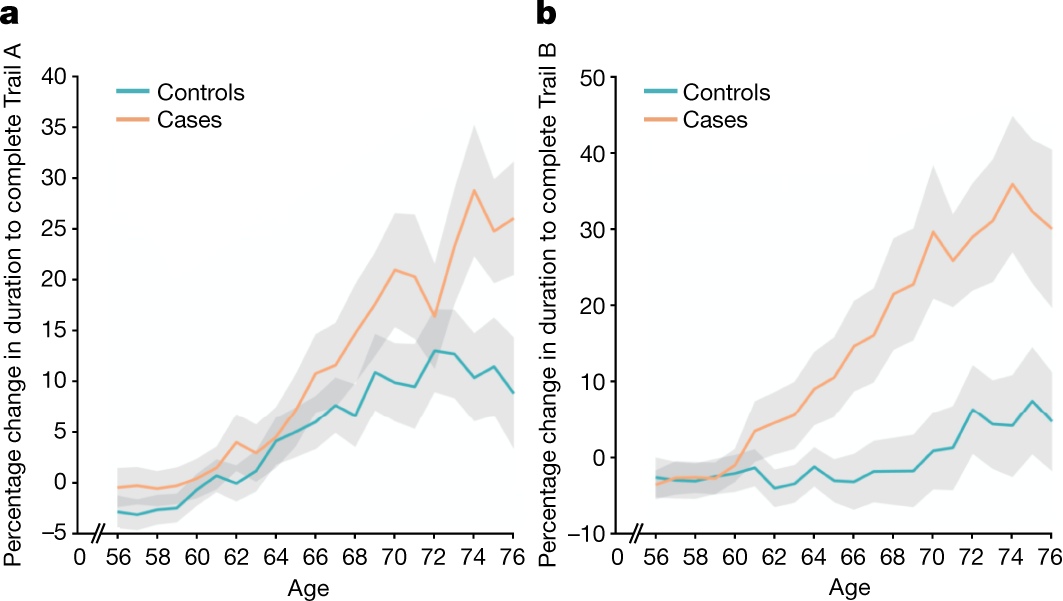
Fig. 3: Significant longitudinal differences in cognition. from SARS-CoV-2 is associated with changes in brain structure in UK Biobank. Shows cognitive impairment by the difference in time required to do a task.
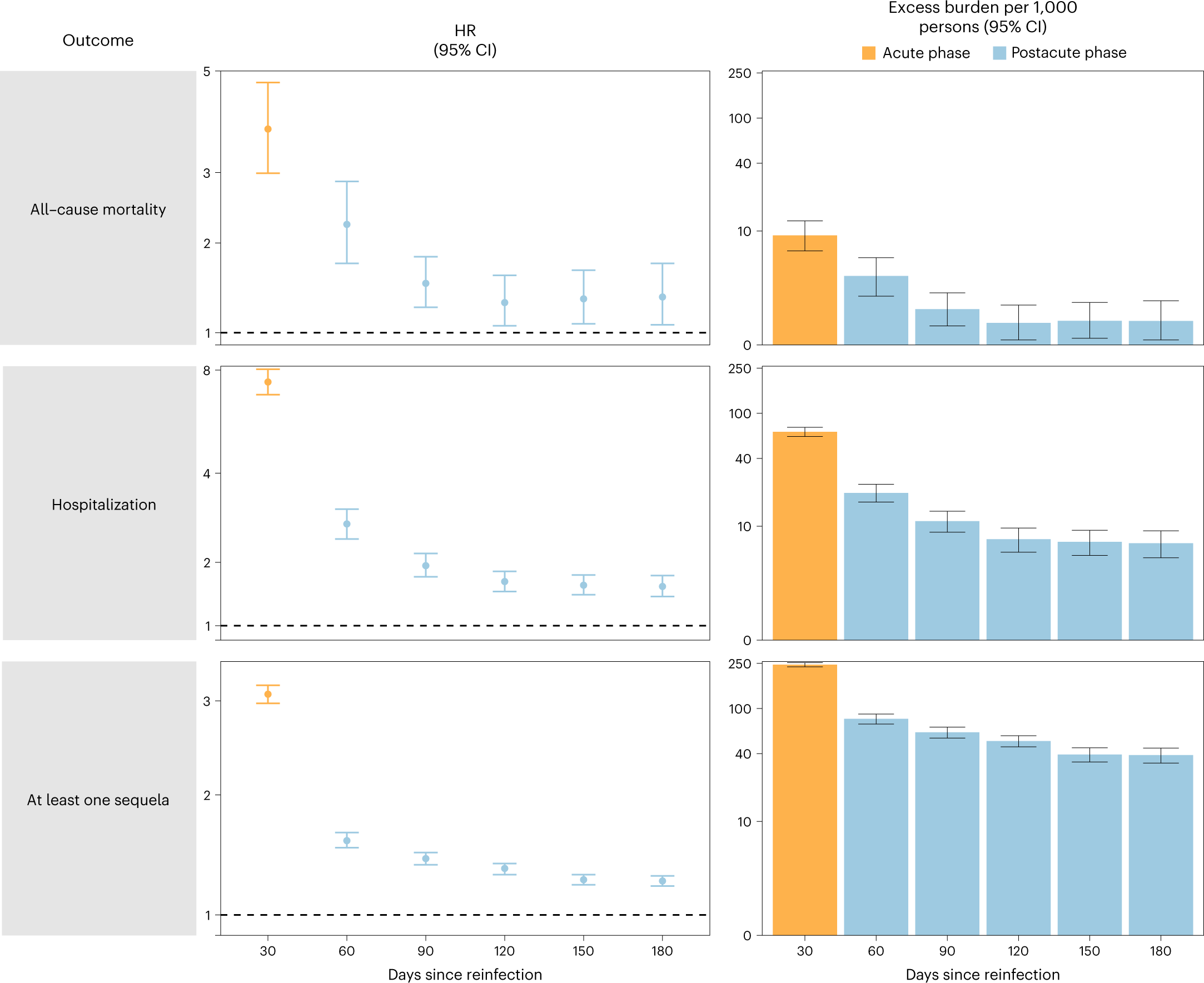
COVID Reinfection is just as dangerous or more dangerous than the initial infection. Source: The COVID ‘acute’ phase doesn’t really end until 90-120 days post-infection. Source: https://www.nature.com/articles/s41591-022-02051-3/figures/3
2) Protect yourself like a Billionaire; get and use HEPA filters, and use COVID tests if you must gather: At the Davos World Economic Forum this year, there were stringent and multi-layered anti-COVID precautions, including masking, improved ventilation and filtration, and mandatory testing with immediate revocation of access on positive test.
The COVID ‘acute’ phase doesn’t really end until 90-120 days post-infection. Source: https://www.nature.com/articles/s41591-022-02051-3/figures/3
The end to COVID may still not be in sight yet, but we now have a lot more information about how to protect ourselves from it, and maybe, just maybe lighten the load on our overloaded and buckling healthcare system. It is possible to get back to the low case counts of mid-2021, we just need to work together and make sensible decisions. Stay safe out there.
The best current study on the dangers of reinfections: “Long COVID after breakthrough SARS-CoV-2 infection”, Nature Medicine, 25 May 2022
Some quotes from the above two references:
“The organ damage experienced by patients with long COVID appears durable, and long-term effects remain unknown.”
“Cognitive impairments in long COVID are debilitating, at the same magnitude as intoxication at the UK drink driving limit or 10 years of cognitive ageing73, and may increase over time, with one study finding occurrence in 16% of patients at 2 months after infection and 26% of patients at 12 months after infection74”
“Few people with long COVID demonstrate full recovery, with one study finding that 85% of patients who had symptoms 2 months after the initial infection reported symptoms 1 year after symptom onset143. Future prognosis is uncertain, although diagnoses of ME/CFS and dysautonomia are generally lifelong.”
“The findings highlight the clinical consequences of reinfection and emphasize the importance of preventing reinfection by SARS-CoV-2.”
Other references and links in-line
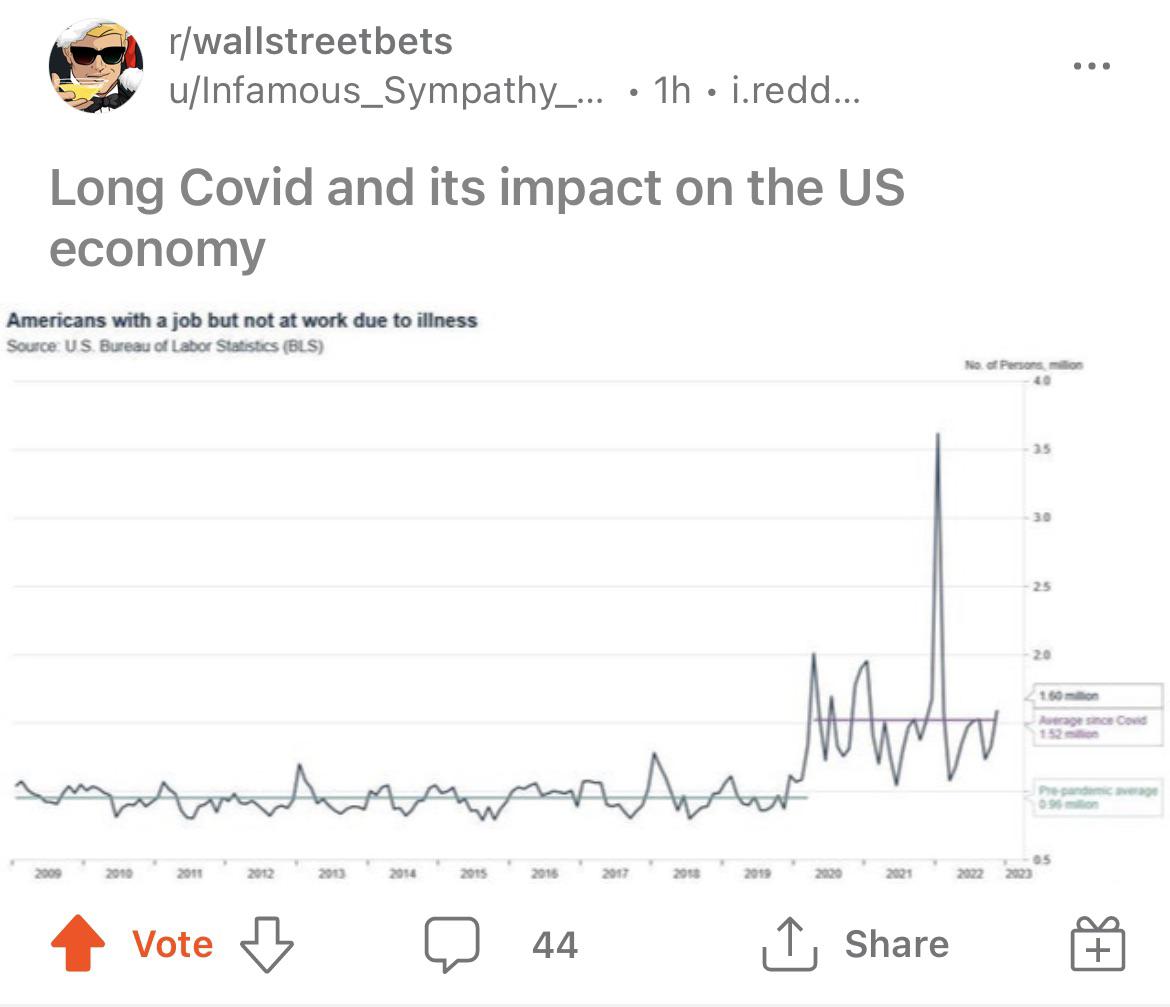
A final word from r/wallstreetbets and the Bureau of Labor Statistics:
r/ Wall Street Bets drawing trend lines on the Bureau of Labor Statistics chart, showing the greatly increased number of people out sick from work in an ongoing way.
[2] Reasons why the number of deaths from COVID is difficult to measure include undercounting for reasons such as due to delayed or incomplete reporting of deaths due to institutional overload, delayed annotation of cause of death, and the fact that ‘coroners’ are a profession with inconsistent regulations and training requirements. Overcounting can occur when a person would have died anyway, or COVID is counted as one of a group of causes of death for that person. For this reason, ‘excess deaths’ are typically used in case of pandemic or war.
[3] ‘Case Fatality Rate’ is generally measured as (# of deaths confirmed attributed to COVID)/(# of cases of COVID detected). Incorrect attribution of cause of death can move this number in either direction (although measuring ‘excess deaths’ can help), and reducing the level of testing can lead to this number being overstated (you can look at the ‘test positivity rate’ to get a sense of how under-tested the population is (or how bad the outbreak is)). ‘Case Fatality Rate’ is generally assumed to be an overstatement of the fatality rate, if there are a large number of undiagnosed cases in the population, which are taken into account in the probably more accurate ‘Infection Fatality Rate’.
Early on in the pandemic, a blogpost came out entitled “Coronavirus: The Hammer and the Dance“. It talked about how, in a pre-vaccine world, to avoid overwhelming our healthcare system, but to allow as much semblance of normalcy as possible, we would need to have successive implementations and releases of various non-pharmaceutical interventions (read: lockdowns, public mask wearing, quarantines, etc.)
As difficult as it was to deal with the reality of that (no matter how much I thought I was mentally prepared for it), it’s perhaps even more tiring now, that in a COVID vaccine world, that with substantial anti-vaccination movements and vaccine hesitancy, and with a new variant (Omicron), that we have to continue this ‘Hammer and Dance’.
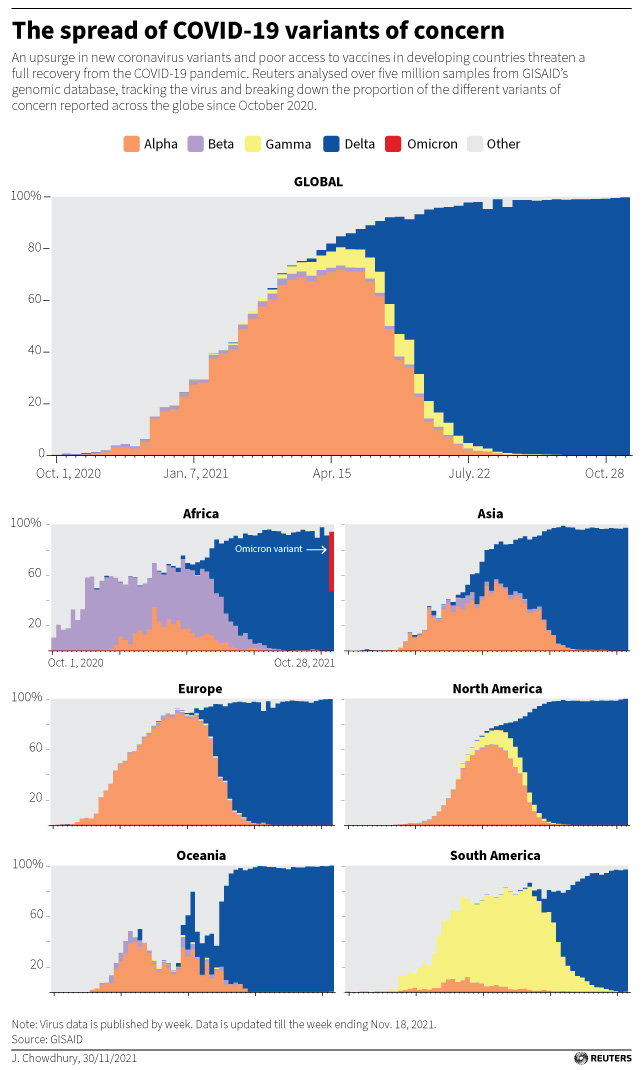
So, that tells you something about the population-wide effects of Omicron, but population effects are equal to individual effects times overall virulence[2]…and what are the individual effects of Omicron, and how is it different from ‘wild-type’, ‘Alpha’, and ‘Delta’?
(Pre-Omicron) Chart showing COVID variant prevalance over time
According to this article, Omicron is 2.7-3.7 more infectious than Delta among vaccinated & boosted individuals, but about the same as Delta among the unvaccinated, suggesting that some sort of ‘immune evasiveness’ is at play.
This article suggests that: “Compared with patients who had the delta variant, omicron patients had a 53% reduced risk of hospitalization, a 74% reduced risk of ICU admission and a 91% reduced risk of death.” (Original paper)
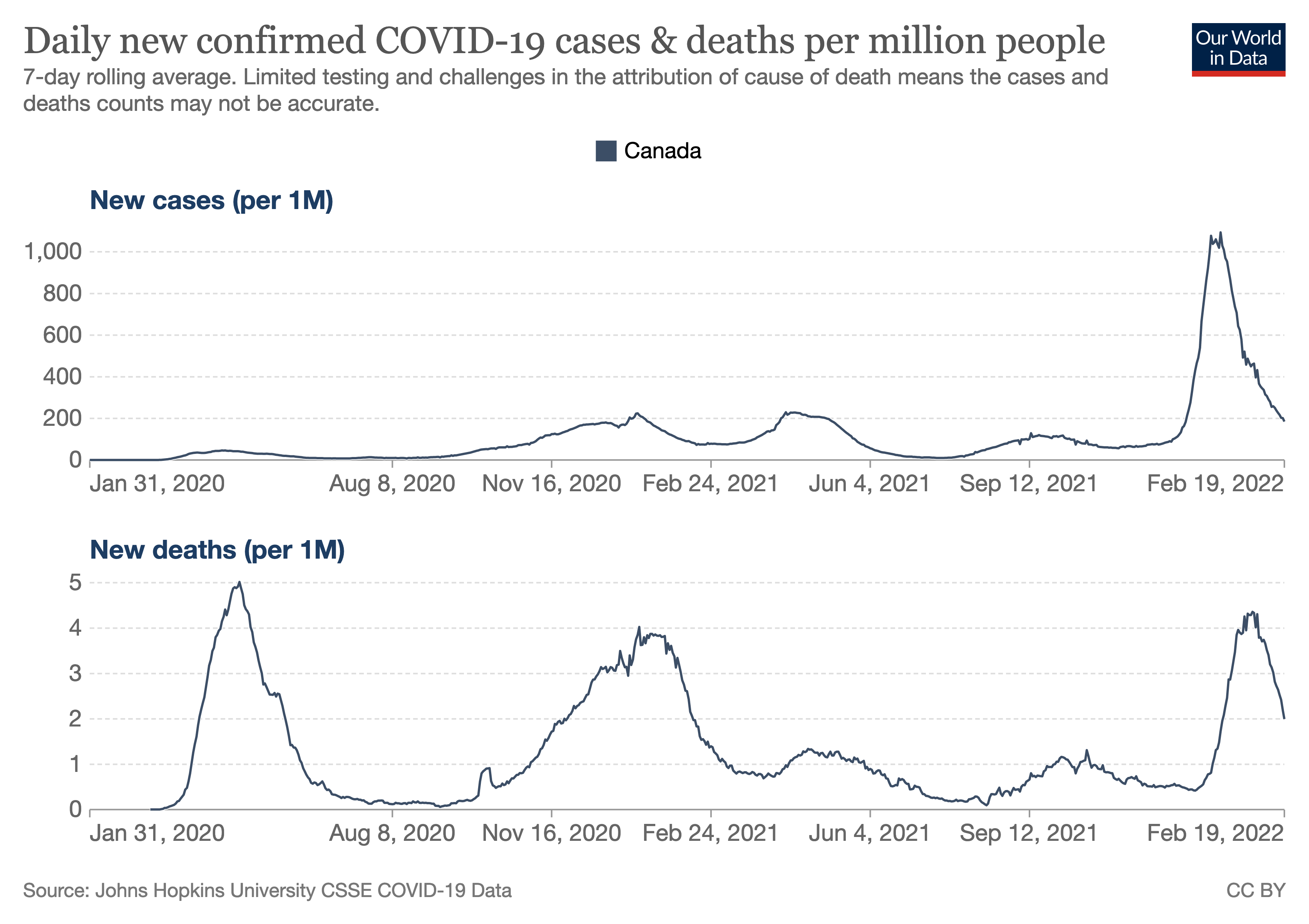
The following chart bears this out:
Chart showing COVID cases and deaths in Canada from the start of the pandemic until Feb 2022.
Here, on the lower chart, you can clearly see the five peaks[5] of the (so far) five waves of the pandemic (in Canada). The first peak, in early 2020, of (probably) exclusively wild-type, hitting the entirely unvaccinated population hard, then a (relatively) calm 2020 summer, followed by the second peak in late 2020 and early 2021 likely brought on by winter forcing people indoors, relaxation of restrictions, and complacency. Vaccines began to be approved in December, and were rolled out through the first part of 2021, blunting the third wave (mostly Alpha) and the fourth wave (mostly Delta) in the fall and early winter. As you can see, the fifth wave was quite different, with Omicron blazing through the population, multiple times more contagious than Delta, but also less deadly on a per-case basis, but overall leading to a wave about as large as the initial first early 2020 pre-vaccine wave.
So, we’ve all heard about the acute COVID symptoms that are included in the above[6], and there have been some issues with people taking a while to recover from these, but more serious, and less talked-about is the phenomenon of ‘Long COVID’ or ‘Post-COVID syndrome‘.
COVID is known to attack the lungs, the heart, the kidneys, and the brain, among other organs.
As a respiratory disease, it is perhaps not unexpected that COVID would attack and damage the lungs. However, much of the attack on organs done by COVID is thought to be because of extracellular expression of ACE-2[7], the doorway that COVID uses to get into cells and multiply.
So, we know that all kinds of things can happen, but how often do they happen? This study, performed in the highly-COVID-tested population Faroe islands, is likely to have included all of the relevant population that contracted COVID (from April to June 2020, so pre-vaccine, all wild type variant). Four months ‘after’ COVID, half of the population studied continued to have at least one symptom (most often fatigue, lost of smell/taste, and/or joint stiffness).
This much larger study of 270,000 people in the U.S. used six months of HMO data, and found that “over 1 in 3 patients had one or more features of long-COVID recorded between 3 and 6 months after a diagnosis of COVID-19. This was significantly higher than after influenza.” In addition, “[f]or 2 in 5 of the patients who had long-COVID features in the 3- to 6-month period, they had no record of any such feature in the previous 3 months.”
”
“You might have a mild case,” Laurie Bedell, 42, of Pittsburgh, said. “But most people that have long Covid had mild cases.”
She caught the virus in December 2020 and continues to have debilitating pain, fatigue and other symptoms that have transformed her from a healthy, physically active woman to a chronically ill person unable to walk or do any form of exercise for more than 5 to 10 minutes at a time.
…
“I am terrified,” she said. “I don’t know that I would survive another infection.”
”
There is currently only anecdotal evidence, but studies are sure to follow, but:
”
People with long Covid “have good reason to be worried, unfortunately,” said Dr. John Baratta, founder and co-director of the UNC Covid Recovery Clinic in Chapel Hill, North Carolina.
“We have seen people in our clinic who have been reinfected with Covid with the other variants,” he said. “They have new or worsened long Covid symptoms after their reinfection.”
”
Third, continue to limit the amount of time you spend sharing air with people outside your ‘bubble’. COVID is an airborne disease, and transmits much more easily indoors, where ventilation is poorer. Consider contactless delivery, masked curbside pickup, and socially distanced and/or masked walk’n’talks.
The end to this thing may or may not be in sight, but it’s probably not Omicron, and you want to get Omicron as few times as possible.
[3] There are limitations on the precision of PCR and the classification of variants, but any study that didn’t do whole genome sequencing would have the same limitations. It increases my confidence in the study that they were very precise about what they were measuring.
Cough
Fever or chills
Shortness of breath or difficulty breathing
Muscle or body aches
Sore throat
New loss of taste or smell
Diarrhea
Headache
Fatigue
Nausea or vomiting
Congestion or runny nose
Some of these symptoms are very common and can occur due to many conditions other than COVID-19, the disease caused by the coronavirus called SARS CoV-2. If you have any of the symptoms, contact a doctor or other health care provider, who can assess your risk and help you determine the next steps.
Emergency Warning Signs of Severe COVID-19 — When to Call 911
If you or someone in your household is experiencing any of the following symptoms, call 911 or your local emergency room right away and let the operator know that you are calling for someone who might have COVID-19:
Difficulty breathing
Persistent pain or pressure in the chest
New confusion
Inability to wake up or stay awake
Bluish lips or face
There are other possible symptoms of COVID-19. Call your doctor or health care center regarding any symptoms that are severe or concerning to you.
”
[7] Angiotensin Converting Enzyme 2, a transmembrane protein involved in blood pressure regulation, and extensively studied because of its relation to hypertension.
[This is a fast-moving and controversial topic, so if you’re reading this, you may disagree with what I say, or I may be wrong. Please feel free to read the sources linked throughout my post. If in doubt, please consult with your doctor. Also, I’m writing this as much for myself, to process all the things that I’ve been hearing and reading, so this may or may not address your specific case. #notmedicaladvice]
By the time you read this, if all goes well, I will have received my first vaccine dose. I’ll be getting the AstraZeneca-made vaccine, for a bunch of reasons, perhaps best summed up by this quote from our Prime Minister:
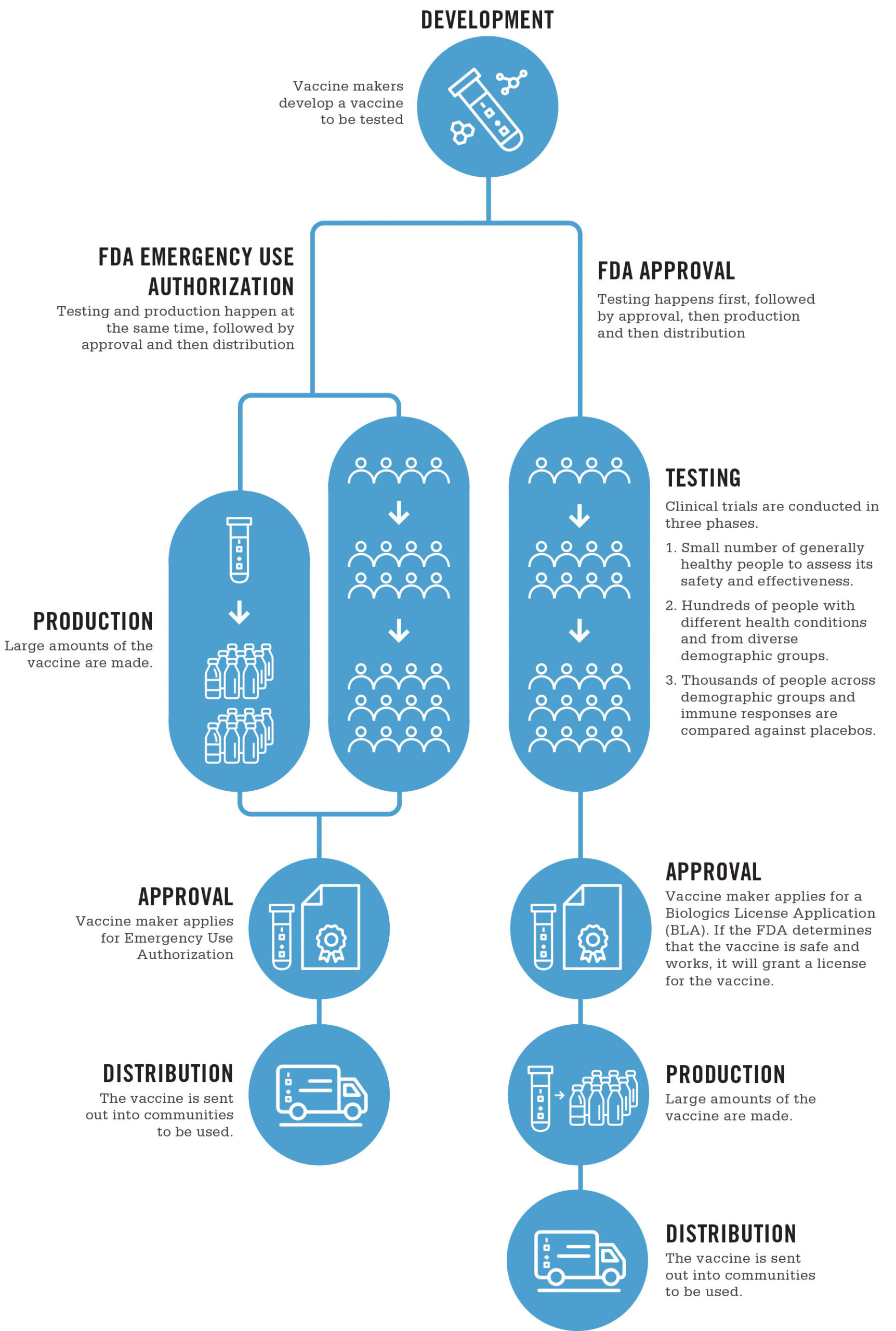
There’s a bunch to unpack here. In order for a vaccine to be offered to anyone, it needs to go through a number of steps, shown in this handy chart from UNC Healthcare:
Infographic from UNC Healthcare showing the FDA vaccine approval process, and how it differs under an ‘Emergency Use Authorization’
1) The initial R&D of the vaccine, including the conceptualization, and very likely in vitro (cell culture) tests and in vivo (animal) tests, both to show safety and effectiveness
2) Three phases of increasingly large clinical trials, to test for safety & effectiveness
3) Formal approval
The above process is the one for the U.S. FDA, but other jurisdictions will have similar processes. In Canada, the National Advisory Committee on Immunization (NACI) does a review of the evidence, and makes an approval decision. As vaccines can have risks as well as benefits, the NACI may approve vaccines for certain demographics, and not others. A common example of this might be restricting approval to adults 18 and over, due the difficulties and ethical restrictions of testing on children. Indeed, the current statement on the AstraZeneca vaccine includes such a statement:
“The AstraZeneca COVID-19 vaccine is authorized for use in Canada for adults 18 years of age and over. Health Canada has determined that it is a safe and effective vaccine.”
The availability of multiple approved vaccines has led to comparisons of the four vaccines currently approved for use in Canada: Johnson & Johnson, AstraZeneca, Pfizer, and Moderna
This being a fast-moving topic, affecting millions (really, billions) of people, science news is being reported on a daily basis in the popular press, which has a number of effects:
Because the topic is fast-moving, there is a lot of news, not all of it checked to normal standards of scientific rigor.
(Apologies for the formatting below, but WordPress is tricky. You may want to rotate your phone to read the table in landscape. The full description of each of the columns is available here, and the names of the columns appears before the abbreviations below.)
Number of adverse event reports by vaccine name up to and including April 16, 2021 (n=3,738) Vaccine name Non-serious reports Serious reports Total reports Total number of doses administered Total non-serious report rate* Total serious report rate* Total report rate*
Non-S Ser Total Total Rate R(ser) R(non-ser)
Pfizer-BioNTech 1,762 395 2,157 7,183,048 24.53 5.50 30.03
Moderna 1,311 83 1,394 1,843,805 71.10 4.50 75.60
COVISHIELD 124 36 160 491,171 25.25 7.33 32.58
AstraZeneca 11 9 20 615,582 1.79 1.46 3.25
Unknown 1 6 7 N/A NaN NaN NaN
* Per 100,000 doses administered.
(‘COVISHIELD’ refers to the AstraZeneca vaccine, under a slightly different brand name.)
Overall, between all the vaccines administered, there have been:
(Please note that this number of 19 per ~9.5 million may go up or down, but as it stands, it’s about at 2 per million, or 1/4 as dangerous as being a pedestrian, or 1/13th as dangerous as driving a car for a year. (2017 data))
(Please also note that all of these vaccines seem to have similar rates of serious and non-serious side effects.)
The item at the top of the news at present is that there are currently specific questions about blood clots and the AstraZeneca vaccine. Health Canada performed a review, and determined:
”
Health Canada’s review of the available information concluded that a link between the use of AstraZeneca COVID-19 Vaccine and COVISHIELD and the risk of these blood clots with low platelets is possible. The risk of these events is very rare, and the overall benefits of the vaccine in protecting Canadians from COVID-19 continue to outweigh its potential risks.
Health Canada did not identify risk factors, such as age or gender, for these very rare events, and is not restricting the use of the vaccine at this time.
A potential mechanism for the combination of blood clots with low platelets is the triggering of an immune response by the vaccine, leading to a condition similar to that seen sometimes in patients treated with the blood thinner medication heparin.
”
In the UK, this incidence seemed to be:
”
The potential risk of blood clots with low platelets is very rare. Based on their vaccination rate as of March 31, 2021, the United Kingdom Medicines and Healthcare Products Regulatory Agency estimated the overall risk of these blood clots to be approximately 4 people in a million who receive the vaccine. Reported cases of these adverse events have been seen after the first dose, usually within the first 14 days after immunization.
”
While the overall population risk seems low, when people have options, they will move to optimize their decisions with whatever information they have available, especially when there may or may not be demographic effects on these issues. At its worst, this leads to ‘vaccine shopping’, exacerbating outbreaks, but at its best, it involves people making educated decisions about their personal risks and benefits from taking a particular vaccine. Indeed, from the NACI April 23rd statement:
“At this time and based on current evidence, NACI recommends that the AstraZeneca COVID-19 vaccine may be offered to individuals 30 years of age and older without contraindications, if the individual does not wish to wait for an mRNA vaccine and the benefits outweigh the risk.”
This represents the fact that individuals between the ages of 30 and 40 are at reduced risk for COVID (compared to older individuals), and they may be at the same or increased risk for these blood clots.
There has been speculation that this is auto-immune linked, but the current (not yet published) research has not found (or ruled out) a link yet. (Numbers are still very small, and this is a tricky determination to make.)
However, if you know that you are more susceptible to auto-immune issues (especially those with high estrogen levels), you might want to consult with your doctor, or wait if it remains safe for you to so, while the science is worked out. Ultimately, only you (with your doctor) can make this determination.
However:
Overall, the title of this post still stands. There are a small number of rare side effects associated with these vaccines (mainly PEG allergic reactions for Pfizer & Moderna, and blood clots for AstraZeneca), both of which are detectable and generally treatable. I’m planning to get my shot tomorrow morning, and I believe that the vast majority should also, as soon as they can.
Stay safe.
-Nayrb 🙂
[1] “The Pfizer-BioNTech COVID-19 vaccine is contraindicated in:
– Individuals who have ever had a severe allergic reaction (i.e. anaphylaxis) to a previous dose of an mRNA vaccine or to any of its components (including polyethylene glycol (PEG) and/or polysorbate) or its container, should not get either mRNA COVID-19 vaccine. PEG can rarely cause allergic reactions and is found in products such as medications, bowel preparation products for colonoscopy, laxatives, cough syrups, cosmetics, skin creams, medical products used on the skin and during operations, toothpaste, contact lenses and contact lens solution. PEG also can be found in foods or drinks but is not known to cause allergic reactions from foods or drinks.
– Vaccination should be deferred in symptomatic individuals with confirmed or suspected SARS-CoV-2 infection, or those with symptoms of COVID-19.
– As a precautionary measure and in light of the need to be able to monitor for COVID-19 vaccine adverse events without potential confounding from symptoms of COVID-19 or other co-existing illness, it would be prudent to wait for all symptoms of acute illness to completely resolve.
– Individuals who have received another vaccine (not a COVID-19 vaccine) in the past 14 days.
– Individuals under the age of 16: The safety and efficacy in children under 16 years of age have not yet been established. The manufacturer plans to conduct clinical trials in children.
Considerations for other patient groups
– Guidance for special populations, including for example breastfeeding or pregnant individuals, individuals with allergies, individuals with autoimmune conditions, or individuals who are immunocompromised due to disease or treatment, is available in the Vaccination Recommendations for Special Populations guidance document.
Precautions during vaccination should be taken for:
– Patients who have a bleeding problem, bruise easily or use a blood-thinning medicine should receive the vaccine. Individuals receiving long-term anticoagulation with either warfarin or heparin are not considered to be at higher risk of bleeding complications following immunization and may be safely immunized through the intramuscular route as recommended, without discontinuation of their anticoagulation therapy.
– There is some evidence to suggest that instramuscular administration may be safer when given with a small gauge needle (23 gauge or smaller) and when firm pressure is applied to the injection site for 5 to 10 minutes
– Individuals with a history of severe allergic reactions (i.e. anaphylaxis) not related to vaccines or injectable medications—such as allergies to food, pet, venom, environmental, or latex, etc. should be offered the COVID-19 vaccines.
– An extended period of observation post-vaccination of 30 minutes is recommended for these groups
– For more detailed recommendations on people with allergies, please consult the Vaccination Recommendations for Special Populations guidance document.
” https://www.health.gov.on.ca/en/pro/programs/publichealth/coronavirus/docs/vaccine/COVID-19_pfizer_vaccine_administration.pdf
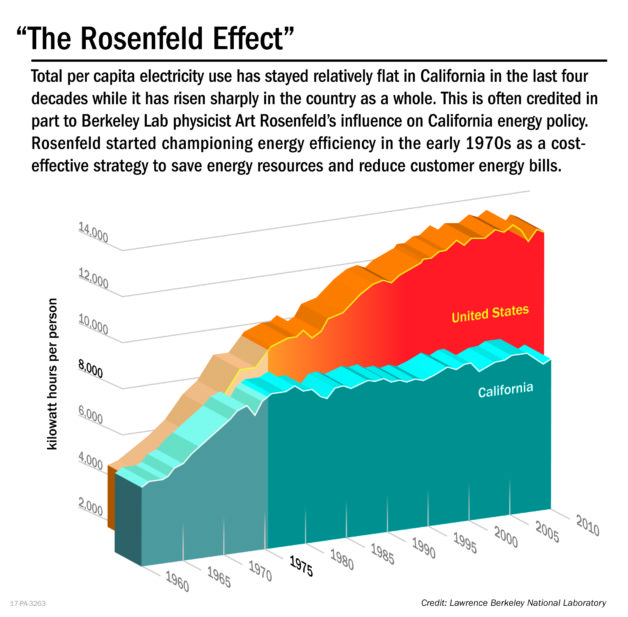
Art Rosenfeld passed away two weeks ago. Most people would not remember him, but they have been affected by his simple observation in 1976 that a “proposed nuclear power plant would not be needed if refrigerators were required to be more efficient.”
Here you can see the effects on the energy efficiency in the state of California:
“The Rosenfeld Effect.”
Note how the energy expenditure per capita flatlines from the time he made the observation above. It was never one thing, but a lot of little things Turning off lights at night, higher efficiency furnaces and fridges and stoves. Higher efficiency lighting. Better windows.
These are the kinds of things which make a huge difference in aggregate (and he was a master at expressing how much of a difference each of them would make singularly, such as spending 20mins with light switches saves 100 gallons of gas over the weekend). These are the kinds of incremental changes which are slowly reducing the scourge of cancer[1]. These are the kinds of things which can reduce changes to the climate.
Thanks, Art. Let’s keep working and doing things a little more intelligently every day.
20 years ago, I watched Contact in the theater with my family[1]. Tonight, I watched it again, with S.
To me, it held up well as a movie. All the characters were believable, and the science and the effects were well within the normal parameters of suspension of disbelief.
What struck me[2] was how hopeful a movie it was, that our better natures would win out, that our endless curiosity would take us places we’ve never imagined.
[Note that spoilers follow]
It’s always interesting the things you remember 20 years later. “Why not make two, at twice the price?” The destruction scene. The prime numbers sounding so ominously alien from the aether. The speaking through her father. The 18 hours of static[3].
Interestingly, I had remembered that 18 hours of static as being the vindication at the end of the movie, that she was not crazy, that something had indeed happened, but I had forgotten how much it was covered up.
The one (gaping) plot hole I had missed the first time around was the absence of study and testing before a human was sent through the machine. If you look at the history of the Apollo program, you see that it was preceded by Mercury and Gemini, with dozens of sequential missions, each testing new parts, to make sure that each part of the system and plan were well-enough understood to ensure successful missions. The idea that they would build a half-trillion-dollar system in Contact and not fully study it (especially if it’s generating strange EM radiation) before sending a human through it ‘strains credulity’. Even the EM it’s radiating would be a fantastic discovery for humans.
But I can understand how they would cut out things to make a move that was watchable, and which was able to spend its time focusing on the humans in the story.
The alternative view of events that the NSA directory was trying to convince people of at the end of the movie was reminiscent (for me) of the big con[4] at the end of ‘Watchmen’, albeit at the opposite end of the hope-fear axis.
Apparently, like Bladerunner, the ending was supposed to keep your doubt alive as to whether the events she experienced had actually happened. To me, it didn’t, as 18 hours of static (and whatever metallurgical data they could get from the sphere) would be enough to prove the story.
I laughed, I cried, I am full of hope. A new year dawns. Time to use that hope to build something meaningful, starting with some words.
[1]We immediately followed it with Men In Black. I’ll leave it to you to enjoy this juxtaposition.
[2]If you’d read or watched any Carl Sagan, this would probably not be surprising. “The sky calls to us. If we do not destroy ourselves, we will one day venture to the stars.”
[3]I had remembered it as 18 minutes.
[4]In ‘Contact’, it was posited that a billionaire had faked first contact to inspire humans to push themselves outwards. In ‘Watchmen’ (the graphic novel[5]), Adrian Veidt fakes an alien invasion to scare humans into working together against a common foe.
[5]’Watchmen’ the movie simplified the plot to have Doctor Manhattan be the scapegoat. this lead to a much tighter movie, but slightly less appropriate for my analogy, however much he played with space and time.
So, a good friend of mine recently posted the following meme:
Depressing thought…But is it true?
“According to astronomy, when you wish upon a star….
You’re actually a few million years late.
That star is dead.
Just like your dreams.”
It’s a really depressing thought, perhaps even more depressing than the Nietzsche/Kubrick mashup: “God is dead, and you are alone in an uncaring universe.”[1]
At least with an uncaring universe, something with persist after you are gone. If all the stars are dead before you can even see them, would there even be anything left after we are gone?
But extraordinarily depressing statements require extraordinary evidence. So let’s take this sentence apart and define some things.
First: “According to astronomy” means that we get to (and have to) use astronomy in our proof or disproof. It also likely refers to modern astronomy, as it did not specify a time/technology period. (It may be interesting to see if any answers would be different under astronomy from a different time period, but that will be a secondary investigation.)
Second: “when you wish upon a star….” has a few different readings. The phrase seems to come (at least most recently) from the song written for Disney’s Pinnochio. In that movie, Gepetto says the following:
”
Look! A wishing star!
Starlight, star bright, first star I see tonight…
I wish I may, I wish I might have the wish I make tonight.
”
But going back to “When you wish upon a star, the meme-maker seems to be clearly referring to the 1940 Disney song and film. Looking at the occurrences of this song in the film:
So, this restricts us to the realm of non-moving (or slowly-moving) celestial objects[4]. From the film, the star also seems significantly brighter than the surrounding stars, but the exact extent to which this is true could be dramatic license.
The rhyme mentions ‘first star I see tonight’, which also suggests that the celestial object seen is unusually bright.
So, non-moving (or slowly moving) celestial objects which are bright. This leaves us with comets, planets, and bright stars[4][5].
Comets are objects orbiting through the solar system, and unless they fall into the sun, impact another body, or otherwise breakup, they tend to go on ‘living’ after we see them. (Halley’s comet has been known since at least 240BC.)
Planets could easily look like stars, often like unusually bright stars. Venus was called the ‘evening star‘[6] since antiquity, and it would be bright enough (up to apparent magnitude -4.9) to be significantly brighter than anything else in the sky. Venus could be considered ‘dead’ because it may have once supported life before a runaway greenhouse effect millions of years ago, but this seems an unlikely metaphorical interpretation. Mercury (up to apparent magnitude -2.45) would also be significantly brighter than anything but Venus (and the moon and sun), but has never been ‘alive’, being too close to the Sun[7]. Mars (up to apparent magnitude -2.91) could have been alive at some point, in the same vein as Venus. One or more of the moons of Jupiter (up to apparent magnitude -1.61) or Saturn[8] (up to apparent magnitude 1.47) could have been home to life, under this same metaphorical definition. (The other planets and other bodies in the solar system are too dim to ever be a ‘bright star’.)
So, a planet could be a metaphorical source for this quote, but this seems unlikely, as the quote seems to be referring to the fact that the celestial object is no longer emitting the light itself.
This leaves us with bright stars. Looking at the brightest star in the night sky, Sirius (up to apparent magnitude -1.46), it[9] is only about 8.6 light years away, so we would know in less than a decade if something were to happen there.
You will note that even the furthest among these, Deneb is still only 2600 light years away, much closer than the ‘few million years’ mentioned above.
Based on all this evidence, it would seem that the original meme:
“According to astronomy, when you wish upon a star….
You’re actually a few million years late.
That star is dead.
Just like your dreams.”
is false, which is good, because it would be super-depressing otherwise.
If you enjoyed this sojurn through astronomy, you may like the rest of my blog. Comment below with things you want me to talk about or investigate!
[1]If you have a better source for this, please let me know.
[2]If you want to be pedantic (and I know you do), you could say that meteors are the dead husks of possible (or tidally destroyed) planets, and their burning up in the atmosphere is hundreds of millions of years after they ‘died’.
[3]Much less than a second, even if you assume they impact the Earth’s atmosphere thousands of kilometers away.
[4]A close supernova might also qualify, as it could easily be brighter than anything else in the night sky, would last just long enough to be a ‘wishing star’, and would have been ‘dead’ for some time before it was seen by a human observer. This might indeed be source of this rhyme, where a ‘guest star‘ could inspire wishing and omens. However, looking at this list of supernovae, any supernova which would have been visible as a ‘bright star’ with the naked eye would be at most tens or hundreds of thousands of light years away, not qualifying for the ‘few million years’ mentioned above. I also personally see supernovae more as a seeding of the galaxy with heavier elements, and thus wishing upon one of these would be wishing that the spreading of heavier elements would inspire life to form elsewhere in the universe.
[5]I see no way that any reasonable person could confuse the Sun or Moon with a ‘wishing star’.